

Customer Safety is our Top Priority.
Safety is imperative and our customer’s eyes are crucial to their work. Q-Optics rigorously measured light that gets to a practitioner’s eyes when using our high quality headlights. Data captured with NIST-calibrated radiometric equipment yielded light levels that are 33 times lower than safety limit guidelines first published by the American Conference of Governmental Industrial Hygienists (ACGIH).
Q-Optics Technical Report
Introduction
Eye hazards due to light exposure are known factors. Thermal burn from welding arcs and laser radiation are two common sources of potential damage to eyesight. Protection from these risks is commonplace and the danger due to direct exposure is understood by the majority of the population. Less known is the long term hazard associated with exposure to blue light, particularly in the range of 400-550nm.

There are multiple eye safety considerations for general illumination sources that are covered in general lamp specification standards [“Photobiological safety of lamps and lamp systems”, IEC 62471 with informative reference to guidelines by the American Conference of Governmental Hygienists (ACGIH)]. These hazards include the actinic ultraviolet (UV), near UV, blue light, thermal, and infrared. The power integrated over time (fluence) is far too low relative to aversion reflex (0.25 seconds) for the LED sources in headlights for the majority of these factors to be any danger. The exceptional case requiring further investigation is the blue light hazard.
The blue light hazard is important in the dental industry due to the wide use of UV curing lamps. Consequently, this industry (driven by the American Conference of Governmental Hygienists or ACGIH) was on the forefront of defining illumination hazards for non-laser (incoherent) sources [D. H. Sliney, “Ocular Hazards of Light, International Lighting in Controlled Environments Workshop (1994)]. These definitions are based on the photochemical retinal hazard due to blue light exposure (photoretinitis) that can lead to macular degeneration with chronic exposure. The guidelines on the thresholds for safe exposure have been stable for at least two decades and are based on animal experimentation correlated to human eye behavior using accident data. In terms of dental applications, the eye safety concern has been extended recently to include dental headlight assemblies that illuminate oral viewing in a number of applications in the industry.
Required definitions
In order to fully understand the blue light hazard, a few definitions are required. The hazard is defined in terms of radiometric quantities (as opposed to photometric quantities). Radiometric quantities are stated in absolute energy, whereas photometric quantities scale energy levels to correspond to the photopic eye response (the luminous efficacy) [http://en.wikipedia.org/wiki/Photometry_(optics)]. It is common with visual light sources for work to be done in photometric units, but due to the blue light hazard definition only radiometric quantities are discussed here. The relevant SI unit for radiant energy is the Joule (J) and for radiant power is Joules per second (J/s or Watts). Watts should be a familiar unit to readers due to specification of the radiant power emitted by light bulbs and other light sources.
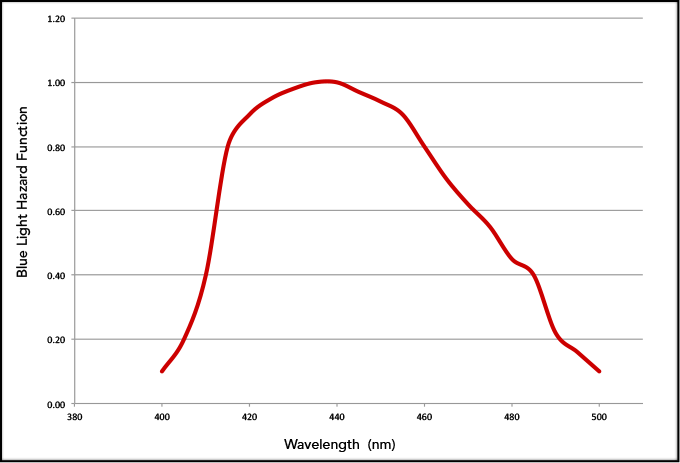
Additionally, energy emitted from a light source can be separated into different wavelengths (in the visible these are different colors). Hence the power emitted at a certain wavelength is called the radiant spectral power. The total power is then obtained by summing the power at all of the wavelengths for the radiation (in other words, integrating the power over the spectrum). In terms of the blue light hazard, different wavelengths pose varying risk to the eye. Hence it is the blue light hazard weighted radiant power that is important, and it is obtained by multiplying the radiant spectral power by the well-known blue light hazard function, shown in the following graphic. The waveband defining the blue light hazard contains wavelengths from 300nm to 700nm (roughly ultraviolet through red).
Thus far the discussion has been around the power emitted from the headlight. What is missing is where the light goes that is emitted. Two quantities are needed to understand where emitted light travels. The first is the area of the emitting source. For a light bulb this is simply the area that is illuminated. If the radiant power is in Watts, this leads to units of Watts per area (such as meters squared, m2) and this quantity is known as the irradiance. This definition also corresponds to light that illuminates an area, such as the light that gets to the pupil of a person’s eye from a scene, or secondary source of light such as the illuminated patient’s mouth. The second important quantity is the angle of emission. We are used to thinking of angle in two-dimensions (a plane), but in three-dimensional space what we a really need is a two dimensional angle (a cone).
The mathematical definition for such a geometric cone is defined as a solid angle and is the area of a cone projected from a point onto a sphere divided by the square of the distance from the projection point to the sphere (area divided by distance squared). More on solid angles can be gathered through common online resources (such as http://en.wikipedia.org/wiki/Solid_angle). The unit for solid angle is the steradian (sr) and emission from a point into a full sphere is 4p sr. A solid angle is needed because not only does energy flow through the area of a source, but it also comes out with a given angular profile and direction in three-dimensional space. The relevant quantity for the blue light hazard is radiance which is the radiant power divided by the product of the source emitting area and the solid angle of emission. Note that if the radiant power is being evaluated at an angle to the source, then the source emitting area is scaled by the cosine of the viewing angle. The units for radiance are Watts per m2 per steradian [W/( m2 sr)]. These fundamental radiometric quantities are covered in a number of common references [such as http://en.wikipedia.org/wiki/Radiometry].
The formal definition of the blue light hazard for an extended source (something bigger than a point of light) is rigorously defined by two scenarios, both using radiance. The scenario is dictated by the brightness of the scene (weighted by the blue light hazard function). In both scenarios, the blue light weighted radiance is calculated. This quantity is the sum from 300nm to 700nm of the spectral radiance times the blue light hazard function times the evaluation wavelength interval (it is basically a discrete form of an integral). Scenario #1 occurs if the blue light hazard weighted radiance is less than 100 W/( m2 sr). The Scenario 1 guideline means that the application is safe for long term exposure to the radiation, specifically for times longer than 10,000 seconds (although for no more than an eight hour period). If this quantity is greater than 100 W/( m2 sr), second scenario in the definition applies. Scenario #2 is the amount of time a user can be continuously exposed (which is a value less than 10,000 seconds), and is defined as exposure time (in seconds) equals 1,000,000 divided by the blue hazard weighted radiance.
What you really need to know — properly quantifying the risk with dental headlight use
The primary discussion on the blue light hazard has been on the relative amount of blue light emitted by dental headlights relative to other wavelengths. Certainly the radiant energy where the blue hazard function is appreciable is a necessary condition for there to be risk. However just looking at spectrum can be quite misleading. For example, a pure blue LED that is quite dim would have a spectral emission that primarily contains blue light, as shown as the blue curve in the following graphic. The implicit second factor is that these sources not only contain blue, but are also very bright. Data are often provided for different sources giving luminous power emitted per unit area (lux or lumens per meter squared). Lumens are the power in Watts emitted multiplied by the eye’s photopic response. Even with the spectrum and luminous flux in hand, there is one crucial missing factor for dental headlights; they are not directly viewed in usage. Rather, dental headlights are used to illuminate a patient’s mouth and the blue light hazard weighted radiance viewed by the eye is the key quantity.
The fundamental standard covering these factors, “Photobiological safety of lamps and lamp systems” (DIN EN 62471 or IEC 62471), gives excellent guidance to properly making blue light hazard measurements. It is known that the radiant power that enters the eye and is absorbed by the retina is dependent on the area of the pupil (the iris of the eye). The standard very explicitly states that the hazard guidance limits for greater than 0.25 seconds use a 3mm pupil diameter. In Q-Optics’ measurements, we used a laboratory pupil diameter that was significantly larger, 11mm diameter. It is worth noting that this is not a significant factor in our results because detection area is factored into irradiance. The light field is reasonably uniform across the detection entrance port in our experiments, where we actively worked to measure the brightest light.

Hence the eye pupil for the vast majority of the population, between 2mm and 5mm in diameter, will yield the same as results as our measurements regardless of where the eye subsamples the field. In bright conditions and with the large amount of other color content in these headlights, such as viewing conditions in the dental office, it is likely 3mm would be the largest pupil size for most practitioners.
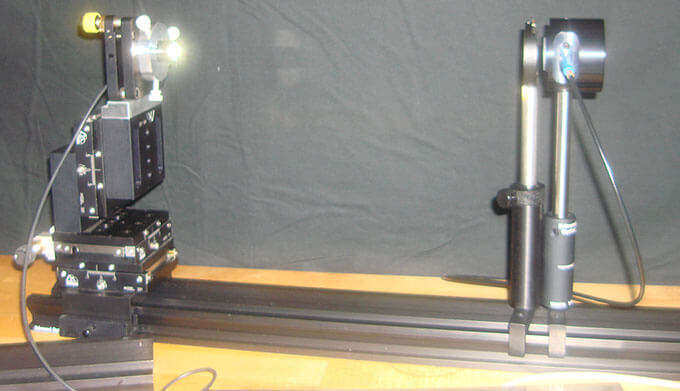
In order to assess the blue light hazard for dental headlights (in this case we used a RADHUM Headlight from Q-Optics), a commercially available irradiance measuring head (Labsphere’s E-1000) was used with a fiber-coupled spectrometer (Labsphere’s CDS-600) in a light controlled environment. This spectral irradiance measurement equipment was absolutely calibrated to NIST traceable standards for the wavelengths of interest to the blue light hazard function (300-700nm). The absolute uncertainty for a given measurement is calibrated to be 10%. An picture of a this equipment is shown in the following graphic, with the headlight source on the left, an iris that used to baffle stray light (the second post from the right), and the irradiance head with fiber readout on the right.
Our Measurement Equipment
A number of measurements can be made using this setup. Direct headlight measurements or measurements of different material reflectance properties varying from specular (such as a mirror) to nearly Lambertian (such as a piece of white paper) are possible. The most significant measurement made was simulating the normal use of the headlight. Namely, we simply placed a patient at an appropriate distance from the headlight with the irradiance head in a position close to where the practitioner’s eye would be located. When this was done we found the risk to be negligible, with the measurements being from 1.2 to 3.0 W/( m2 sr),depending on distance. We did enough experimentation to verify the repeatability of these results under realistic conditions. Our measured radiance is only 1/33rd of the published guideline limit.
We also worked to simulate the effect of tools such as a tooth mirror or Minnesota retractor. It is possible for these tools occasionally have glint that gets to the eye. We also did measurements for different instruments and found that it would take 5-7 minutes of exposure (using Scenario 2) to be at the blue light hazard limit, and these values were obtained by directly shining reflected light into the irradiance detector. With a reasonable 0.25 second aversion response, this would mean that these events would need to happen over 1000 times during a workday, which is improbable. If such annoying events occurred that often these popular dental headlights would not be so pervasive. These instruments are simply not used to shine light from the headlight into the eye.
The final factor for consideration is the effect of loupes. Loupes are commonly used to magnify what the practitioner is seeing. If a user looks at a bright spot of light in a loupe, it will appear larger. For loupes common in the industry, this gain in brightness would be a factor of about 3-7x. Because our direct measurements range from 1.2 to 3 W/( m2 sr), this still would lead to blue light-weighted radiance that is just over 1/5th of the hazard, worst case with high magnification and short working distance (like 10”). This result is also intuitive if you view a patient illuminated with a headlight with and without a loupe.
Concluding remarks
Our findings are that the blue light hazard for proper use of dental headlights is negligible, approximately 33 times less than limits established by the ACGIH over two decades ago. Our results take account of the fact that the practitioner is viewing light return off a face and teeth, where the majority of the blue light is absorbed (because tissue is red) and non-specular as teeth may be glossy but do not return a lot of light (you cannot see yourself reflected in them). This result is not a surprise to illumination experts. Moreover, it is common feedback from customers using these lamps at an ergonomic working distance to want more light due to the low level of light return to the eyes and the fact headlight beams have built-in divergence.
One simple assessment can be done visually at the correct working distance. First look at the headlamp somewhat directly (start far off and move gradually into your field of view). It will most likely not be possible to view the headlight directly, as it is very bright and eye aversion is almost assured. Look at the headlight close to a piece of paper; then increase the distance between the headlight and the paper, note how the spot appears less bright as you move away. In the case of paper, which is nearly Lambertian, a lot of the light is scattered in a hemisphere. Then view someone’s face with their mouth open, as a dental practitioner would, as shown in the following graphic. You will notice that the amount of light in the last case looks far less blue and dimmer, so the results we have gotten make intuitive sense.
The bottom line is that there is a big difference between directly viewing a source, such as a dental curing lamp, and viewing light from an illuminated scene where much of the blue light is scattered or absorbed. The risk with proper use of Q-Optics headlights has been measured to be negligible.